
By Dr. G. John Mullen
Originally posted October 31, 2014
Every swimmer knows breaststrokers are odd characters. When I’m working with any team, I screen their athletes, finding their specific injury risk. During this screen I have my tests for most swimmers, then for breaststrokers… The breaststroker screen caters around the hips and knees more than the other strokes, as the legs provide the bulk of propulsion during breaststroke.
During my screen, I assess hip internal rotation, the main contributor to an elite breaststroke kick. I frequently find swimmers, especially those who aren’t good at breaststroke, lack hip internal rotation. This isn’t a shocking finding, as swimmers and coaches have noticed this for years and given one solution: W-Sitting.
Although W-Sitting is just getting backlash, many in the rehabilitation world have known W-Sitting is hazardous for years.
Here are some problems with W-Sitting:
1. Hip Labral Irritation
The labrum is the protective lining in the hip joint, acting as a rubber seal to help hold the ball hip bone in the socket. When someone sits in the W position, they place a high amount of pressure on the inside aspect of the labrum. Unfortunately, this area of the labrum is the thinnest and most susceptible to injury.
2. Hip Dislocation
The W-Sitting position also pushes the hip range of motion to its limits, increasing the risk of dislocation or subluxation, both during the stretch and afterwards.
3. Medial Knee Injury
During W-Sitting, the medial aspect of the the knee is also stressed. Unfortunately, this increases the risk of medial meniscus and medial collateral ligament injuries, once again, during and afterwards. The medial compartment is already overused in breaststroke swimmers, as breaststroke kicking does stress the area. This also increases the risks of patellofemoral pain syndrome (PFPS) as it creates muscular imbalances perpetuating the risk of breaststroker’s knee.
4. Poor Development of Core Muscles
This is mainly an issue when young children W-Sit, as they often rest more on the passive structures (bones), compared to their active structures (muscles). This decreases the muscular activity during sitting and development. The consequence for poor core development is multi-factorial, with poor performance and low back pain the main issues.
What Allows Hip Rotation?
First, coaches and swimmers, breaststroke kicking is mainly a hip motion! We need to stop stressing the knees and kicking from the knees. This goes for those who have a wide or narrow kick! Instead, drive and kick from the hips! This simple teaching point will greatly reduce the amount of knee pain and develop more hip range of motion if implemented early enough in a swimmers career. The human body is amazing and if a person moves through the range of motion as a youth, their body structure will adapt. Specifically, if a swimmer performs breaststroke properly (from the hips) during maturation, their hip will under go anteversion, moving the femur (upper thigh) forward. This occurs at the shoulders and is one reason why swimmers have so much shoulder mobility. Unfortunately, less swimmers develop hip range of motion for elite breaststroke than shoulder rotation, which I believe is from poor teaching and understanding of swimming biomechanics!
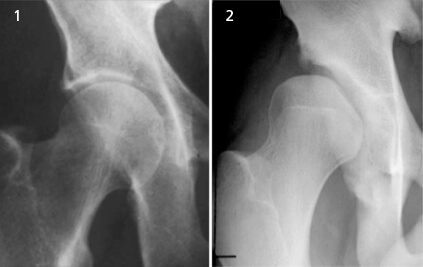
Second, anatomy and genetics do play a role. I never like to bear bad news, but some of you aren’t meant for breaststroke (at least a wide breaststroke kick) and you may not find this out until maturity. Scientific literature is finding out some people have deeper hip sockets than others. A deep hip socket prevents the amount of hip internal range of motion and breaststroke kick width. Japanese have shallower hip sockets, which is potentially why they have a higher rate of elite breaststroke swimmers.
Another anatomical factor is the angle of head of the thigh, the angle of inclination. If you have a smaller angle of inclination, you likely can perform more hip range of motion for breaststroke. Once again, the anatomy plays a role, as different anatomy allows greater motion. If you have a deep hip socket with a large angle of inclination, you pelvis bones likely run into each other, preventing a wide breaststroke kick.
What can we do Other Than W- Sitting?
Luckily, there are many ways to enhance hip rotation without the hazardous W-Sit. Try these three things and enhance your hip internal range of motion today!
- Concentrate on correct breaststroke kick biomechanics, especially at a young age! See above.
- Perform active hip range of motion exercises outside of the water. Simple dynamic warm-up exercises like “Gate Openers” are a simple method of restoring hip rotation outside of the water, as well as improve coordination of this movement.
- Perform self myofascial release (SMR) to the piriformis, tensor fascia latae (TFL) and other muscles limiting hip rotation. SMR are techniques believed to release muscle tension and enhance range of motion. Try these before hopping in the water.
Summary
The rate of knee pain in breaststroke is ~70%. As a swimming community, we should do everything possible to reduce this rate, as it will increase the healthy swimmers in the sport, generating more revenue for swimming, maximize each swimmer’s potential, and improve life-long health, reducing medical costs. Everyone in the swimming community must evaluate the risks of W-Sitting and the benefits. Now, we all know people that can W-Sit without any pain or irritation, but these are likely the anomalies. The Ed Moses’ or Brendan Hansen’s can certainly W-Sit without pain and irritation, but these are the 1/1,000,000!
As I outlined, I see little benefits of W-Sitting which can’t be achieved (and from my experience enhanced) with other, safer methods.
Do your part and keep a swimmer healthier today!
Great article! Is there a video of the correct breaststroke kick on YouTube or anywhere?
Without having done a big analysis, here seems like a good underwater view of Kitajima: http://youtu.be/sDaLdqQwPco
Great article. The video showing SMR didnt really describe the placement of ball. I would like to better understand where to place the ball in order to increase my hip internal rotation.
Here is a post with more information on the TFL:
https://www.youtube.com/watch?v=uZurolGzvyE&feature=youtu.be
Nothing about the TFL is easy and finding it isn’t an exception. The best method to find the TFL is to grab your pelvis with your thumbs facing forward. The top of the TFL is directly behind your thumb and the whole muscle is about one inch wide and two inches long.
For more information, consider purchasing Mobility for Swimmers: http://www.swimmingscience.net/2014/01/mobilityforswimmers.html
Are there videos of incorrect breaststroke kicks to avoid?
Hmm, I couldn’t find any easily online. Nonetheless, here is a pretty good video (IMO) on proper breaststroke kick:
Thank you for sharing! I’ve always been against this ever since I started coaching.
Leah Mulvehill…..
Mackenzie Logan
Zach Kayser
Emmet Crowley
Lies..
Olle Williamsson
Då vet man de ??
Hahaa du som gör det hela tiden ?☺️
Erin Braden Goss Virginia Carr
LOL I would never. Could never.
Yep! Eliminated this one from our dry land program back in the 70’s, more than 40 years ago.
Ole Jørmeland
Trond Vasslag
Beldagans Plus Grace Gutier Mariana Navarrete
Hannah BrunzellAndréa Persson
Somehow hockey goaltenders make it work
My breaststroker a knees just replaced do whatever it takes to avoid that!
I did this for years….never had a problem. BUT I don’t encourage my swimmers to do this, some do some don’t……none have had any issues.
Jessica Hefford
Reni si me detyronte presori ta beja kete ushtrimiiiin ????
Tek ty me shkoi mendja kur e pashe sot. Po une qe e bera te premten ne palester?
Not anymore.
Hahahaha refleksi! Edhe une në fund kur beja stretching e beja kete ushtrimin. Not anymore! Hahahaha
Mac Faldet. Noah Faldet. Read this.
Alexis Mattson
The correct response to this is YET! No problem yet!
Elton Teng
Connor Michie
Tom Olav Bellikka??
Lisa Doufrain
Alison Tallen!
Maik Zeh !!!!
Marissa Hon, Audrey Chong