Guest contribution by Rod Havriluk, Ph.D. Swimming Technology Research; Ted Becker, Ph.D., R.P.T., Everett Pacific Industrial Rehabilitation; Jim Miller, M.D., FAAFP/Sports Medicine, Family Practice Specialists of Richmond, P.C.; Scott Rodeo, M.D., Sports Medicine and Shoulder Service
TALLAHASSEE, Florida, May 4. A recent article in Swimming World (Stott, 2012a) examined “the premise that mega-yardage is a requisite for distance swimming excellence.” In a second article, Stott (2012b) explained the performance benefits of an emphasis on quality with less volume. While the second article may encourage some coaches to avoid excessive training distance, others may be persuaded from the first article that a “history of heavy volume” is typical and quite probably necessary.
For coaches tempted to maintain or even increase training distance, it is critical they are aware of the medical concerns associated with mega-yardage. Improved performance may accompany increased/excessive training distance, but so will shoulder injuries. For example, one study (Richardson, Jobe, & Collins, 1980) reported that elite swimmers (with a higher training volume) experienced shoulder pain at almost twice the frequency of non-elite swimmers. Shoulder injuries are already approaching epidemic proportions (e.g. Haupenthal, et al., 2006; Rodeo, 2011), so extreme care must be taken to reduce the associated risk factors.
There are three generally recognized risk factors for shoulder injuries — muscular imbalances, harmful technique, and overuse (from excessive training distance). As virtually every swimmer has more developed musculature on the front of the body than the back, anterior-posterior imbalances are almost universal. Research shows that shoulder-stressing technique is equally common, as found in 100% of a sample of university butterfliers (Becker & Havriluk, 2010) and 94% of freestylers (Havriluk & Becker, 2012). While any one risk factor can result in injury, and two factors are usually present, overuse (i.e. mega-yardage) adds the third factor for the “perfect storm” effect. Because swimmers are, therefore, both anatomically and biomechanically predisposed to shoulder injury, it is essential that any mega-yardage program include preventive measures and be ready to refer to conservative medical treatments and, in rare cases, surgery.
Screening for and Correcting Muscular Imbalances
A comprehensive approach to preventative measures includes a preliminary screening for muscular imbalances. Coaches can develop a “trained eye” by looking at the symmetry of the muscle structure of the shoulders from front, back, and side views. Bilateral (left/right) symmetry of the shoulder and chest muscles is assessed with the front and back views. Swimmers who rely more on one arm will have a noticeably larger muscle size – indicating a need for technique corrections and developmental exercises. Front/back (antero-posterior) symmetry is assessed with the side view. When the muscular development is greater on the chest versus the back, there is a rounded or forward shoulder appearance. Typically, this forward shoulder appearance will elicit parents to encourage their swimmer to “stand up straight,” which is posturally helpful, but in reality an indication that developmental exercises must be included in a dryland program. Additionally, a trained clinician or physician may use the swim stroke pull test (Becker & Havriluk, 2006) to identify the muscular imbalance (Figure 1).
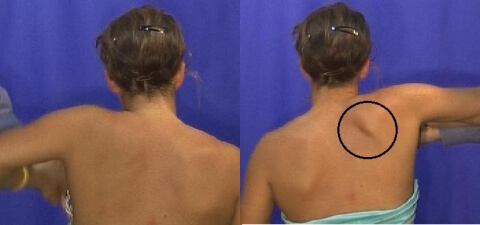
Figure 1. Screening for muscular imbalances with the swim stroke pull test. Note the position of the right scapula.
There are various exercises for preventative and curative interventions. Exercises that strengthen the posterior shoulder muscles are particularly important as muscular imbalance between the anterior and posterior shoulder is typically a precursor to shoulder injury. In one exercise, the fists are close together with the elbows bent at 90 degrees next to the sides of the body at the waist (Figure 2, left). The fists slowly move apart (middle) by outwardly rotating the upper arms as far as possible (right). A partner applies accommodating resistance to match the strength of the swimmer throughout the range of motion.
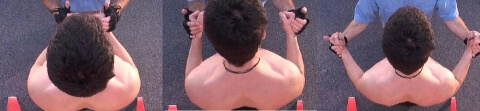
Figure 2. Exercise to strengthen the posterior shoulder muscles.
The best results from this exercise occur when the elbows remain close to the body at the sides of the waist. As the upper arms rotate outward, the swimmer should focus on squeezing the shoulder blades together. The exercise is performed in a slow smooth rotation for one set of 35 repetitions or 3 sets of 2 minutes duration. It is not advisable to use rubber bands because as the band stretches resistance increases and the arm strength is weakest at the end of the rotation.
Screening for and Correcting Harmful Technique
The typical freestyle arm entry stresses the shoulder. The arm usually enters with a very shallow angle so that at the completion of the entry phase the hand is closer to the surface than the shoulder (Figure 3, left). The angle at the shoulder reduces the space for the soft tissue between bones of the upper arm (humerus) and shoulder (acromion), causing irritation and decreased blood flow to the rotator cuff tendons. This position is known as “impingement syndrome.”
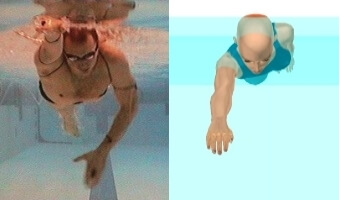
Figure 3. The right arm position at the completion of entry: typical (left) and less stressful (right).
Modifying the arm entry with a downward angle (Figure 3, right) positions the hand deeper than the shoulder at the completion of the entry (Havriluk, 2011). The resulting arm position is stronger (more mechanically advantageous), and most importantly, less stressful on the shoulder.
In addition to arm position, there is also an arm coordination issue related to shoulder stress (Havriluk, 2012). If the arm is held motionless in front of the body as the opposite arm recovers (as in catch-up stroke), the ensuing torso rotation will further stress the shoulder (Figure 4, left). While the typical arm entry position is stressful, an ineffective arm coordination increases the “time of exposure” to the stressful position.
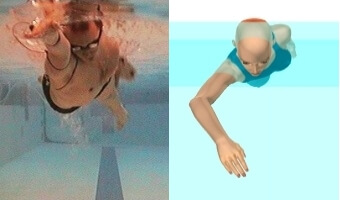
Figure 4. The right arm position at the beginning of the pull: typical (left) and effective (right).
Eliminating (or at least minimizing) catch-up coordination (by immediately beginning the pull after completion of the arm entry) is another way to prevent shoulder injuries. An effective strategy is to immediately flex the elbow as soon as the arm entry is completed (Figure 4, right).
Conservative Medical Treatments
Once injury symptoms such as pain begin, reversing the process while continuing to swim is difficult. At that point, inflammation and musculo-tendonous imbalances are present, leading to pain. The athlete will attempt to compensate by accommodations in technique, which may complicate recovery and slow performance even more.
There are several methods of conservative management once injury is manifested. Hopefully these methods can avoid more serious interventions.
Physical Therapy. Ideally, the therapist should be swimming savvy to appreciate the demands of the sport. Therapies to address inflammation and injury healing include ultrasound, electrical stimulation, laser therapy, deep massage, ice massage, and hydro-massage. The therapist should also recommend and supervise exercises designed to overcome the imbalances and weaknesses that the injury reveals. While there are several options for reducing inflammation and remedying imbalances through physical therapy there has to be an adjustment in the training program for the recovery efforts to be successful.
Massage Therapy. This resembles physical therapy in the manual techniques that are used to assist in recovery by improving blood supply to the injured area as well as to decrease fibrous scar tissue development and regain range of motion. Massage therapy can also be successful, like physical therapy, in correcting muscle imbalances and tightness in opposing muscle groups that stabilize the shoulder or other area of injury.
Injection Therapy. There are several types of injections that can used in the treatment and rehabilitation process. Injections present potential risks, including injury from the injection itself, infection, and tendon ruptures (a known potential complication to steroid shots). Platelet rich plasma injections have also been one of the more recent options, but controversy as to their effectiveness continues. At this time, the only really practical option is corticosteroid, which has an anti-inflammatory effect. There are more injection options and more are likely to be introduced, but they do have risks and warnings, including a need to have the injected compounds investigated against the World Anti-Doping Agency lists of accepted medications.
Acupuncture. Despite the use of small needles, acupuncture is not considered an injection. It works to block pain pathways and improve function and comfort.
Medication. Medication can be taken orally, applied to the skin, or injected. Various injuries respond better to some delivery systems than others. However, most medications are aimed at improvement in discomfort. Rarely will a medication improve healing and in some cases blocking the discomfort may give a false sense of security by depriving the athlete of feedback from their own warning systems. Thus, medication can have an important role in helping symptoms and improving function, but it has to be considered as a piece of the big picture in healing an injury and returning the athlete to full performance potential. Whatever medication is proposed, by any delivery method, it must be checked on the WADA (in the US the USADA) website for the medication's status as allowed, banned or conditionally allowed with a Therapeutic Use Exemption form.
For maximum benefit to the swimmer, all of these methods require coordination of efforts between the medical team, the coaches and the athlete.
Surgical Intervention and Rehabilitation
Most cases of shoulder pain will respond to a comprehensive rehabilitation program. In athletes with pain that persists despite the conservative treatments, the physician should consider unusual sources of pain, including tumor and cervical spine problems. A thorough physical examination with attention to shoulder motion, stability, strength, scapulothoracic mechanics, and the cervical spine should be done. Magnetic resonance imaging (MRI) may be considered to evaluate the shoulder capsule, labrum, and rotator cuff. Athletes with shoulder pain that persists despite training or stroke modifications, rest, and rehabilitation may eventually need to consider surgical intervention.
The persistent pain in swimmers who fail to improve with strengthening is believed to be due to altered shoulder function that results from the combination of muscle weakness/fatigue and underlying laxity. Surgery can be used to address the laxity. Surgery in “swimmers shoulder” typically involves some degree of capsular tightening, which can be done either arthroscopically or via an open incision. The typical rehabilitation phase following surgery involves a physical therapy program. Gentle sculling can start between 8 and 12 weeks, with swimming at 3-4 months, and return to regular training at approximately 6 months.
Conclusions
While there will be always be stress on the shoulder because of the nature of the overhead arm action, controlling the arm entry position and coordination will minimize stress at a critical point in the stroke cycle. Screening for, correcting, and continuing to monitor muscular imbalances is essential. If injury develops, relief may be found from a number of conservative measures before resorting to surgery.
Hopefully, the article on “The Case for Less Volume” in the March issue of Swimming World (Stott, 2012b) will encourage coaches to consider reduced volume options. However, proponents of mega-yardage may be reluctant to abandon a training approach they found successful. A swimmer in a mega-yardage program is likely to perform 1 to 2 million strokes of each arm per year (depending on body size, effectiveness of technique, and swimming speed). Swimmers training far less distance will still perform a huge number of arm cycles. Because of individual differences in shoulder structure and function, some individuals training relatively modest distances may also be at risk.
While the prevention strategies described in this article are imperative for swimmers in high volume programs, swimmers in all programs can benefit. Coaches can screen for muscular imbalances and harmful technique, but because both risk factors are so prevalent it makes sense to include correction strategies in any training program.
References
Becker, T., & Havriluk, R. (2006). Bilateral and anterior-posterior muscular imbalances in swimmers. In J. P. Vilas-Boas, F. Alves, A. Marques (Eds.), Biomechanics and Medicine in Swimming X. Portuguese Journal of Sport Sciences, 6(Suppl. 2), 327-328.
Becker, T. & Havriluk, R. (2010). Quantitative data supplements qualitative evaluation of butterfly swimming. In P-L. Kjendlie, R. K. Stallman, & J. Cabri (Eds.) Biomechanics and medicine in swimming XI (pp.314-316). Oslo: Norwegian School of Sport Science.
Haupenthal, A., Schutz, G., Rushel, C., Faquin, A., Menezes, F., & Pereira, S. (2006). Injuries Incidence in Brazilian Swimmers of Different Strokes. In J. P. Vilas-Boas, F. Alves, A. Marques (Eds.), Biomechanics and Medicine in Swimming X. Portuguese Journal of Sport Sciences, 6(Suppl. 2), 333-336.
Havriluk, R. (2012). Do expert swimmers have expert technique? Comment on “Arm coordination and performance level in the 400-m front crawl” by Schnitzler, C., Seifert, L., & Chollet, D. (2011). Research Quarterly for Exercise and Sport, in press.
Havriluk, R. (2011). Shoulder injuries in swimming: Technique adjustments for prevention and rehabilitation. Paper presented at the USA Swimming Sportsmedicine and Science Network Meeting, Jacksonville, FL, September.
Havriluk, R., & Becker, T. (2012). Mechanical advantage and hand force generation in freestyle swimming. Manuscript in preparation.
Richardson, A. R., Jobe, F. W., & Collins, H. R. (1980). The shoulder in competitive swimming. American Journal of Sports Medicine, 8(3), 159-163.
Rodeo, S. (2011). Shoulder Injuries. Paper presented at the USA Swimming Sportsmedicine and Science Network Meeting, Jacksonville, FL, September.
Stott, M. (2012a). The Case for Volume. Swimming World, 53(2), 26-27.
Stott, M. (2012b). The Case for Less Volume. Swimming World, 53(3), 29-30.
Author Notes
Rod Havriluk is president of Swimming Technology Research. Ted Becker is founder of Everett Pacific Industrial Rehabilitation and was the head trainer for the 1984 US Olympic Swim Team. Jim Miller is a family practice physician and has served as national team physician for USA Swimming. Scott Rodeo is an orthopedic surgeon and team physician for the 2004, 2008, and 2012 US Olympic Swim Team.